Xenon — Anesthetic from Air

Xenon is an inert gas that has no odor or color, does not burn, and is not explosive. It is 4 times heavier than air, almost insoluble in water, and very weakly soluble in oil. In the human body, xenon does not undergo changes, does not enter into biochemical reactions, and is quickly eliminated through the lungs. Xenon is contained in air in very low concentrations — in an average-sized room there is only 4 ml of xenon.
The first report on the narcotic properties of xenon was published by Professor of the Naval Medical Academy N. Lazarev, who in 1946 in experiments on animals confirmed the presence of narcotic properties in xenon (Xe)[55]. Cullen and Gros in 1951 first applied xenon in clinical practice as an anesthetic agent, but only almost half a century later in 1999 did Russia become the first country to officially authorize the use of xenon anesthesia.

There is sufficient convincing data to consider xenon the best of known anesthetics. Xenon is non-toxic, does not have teratogenic and mutagenic effects, does not exert embryotoxic action, lacks allergenicity and carcinogenicity. If we compare the list of requirements for an "ideal inhalation anesthetic," xenon practically fully meets these requirements.
However, the high cost of xenon production constrains the widespread adoption of the method. The price of 15–20 liters of xenon, which is the minimum amount of gas needed for a 2-hour operation, is 75–120 dollars.
Xenon is 1.5–2 times more potent an anesthetic than nitrous oxide. Just 5–6 breaths of xenon in narcotic concentration are enough for a person to experience heaviness in the legs and numbness, gradually rising from bottom to top, affecting the abdomen, chest, neck, and head. At 2–3 minutes, euphoria and increased psychomotor activity appear, with a surge of joyful emotions and a feeling of bliss. Logorrhea (speech incontinence, talkativeness) occurs along with the desire to talk about pleasant sensations. Gradually, stiffness and inhibition increase, and at the 4th minute, a stage of complete analgesia and partial amnesia begins. Five minutes after starting to inhale xenon, consciousness is switched off and the stage of surgical anesthesia begins.
Recovery from anesthesia is rapid. 2–3 minutes after turning off the gas, the patient regains full consciousness with pleasant subjective sensations.
Xenon can be used in closed rooms with limited air circulation, as it does not accumulate in the body, and gas distribution in the room can be calculated using mathematical modeling methods.
Xenon overdose does not require antidotal or even usual drug therapy, is sufficient to provide access to fresh air or oxygen[7,8].
Intelligence interest in the narcotic action of xenon can be traced from the early 60s, when it was first mentioned in CIA documents for the MK-Ultra behavior modification program[19]. At courses of the Ministry of State Security of the DDR (Stasi) on special means, its possible application was also considered[20].
The use of xenon as a "knockout gas" during special operations is unlikely, as the risk of respiratory depression when using narcotic concentrations is too great. Nevertheless, xenon content in air above 0.005% in a closed room can cause lethargy, drowsiness, and coordination disorders in humans. Sub-narcotic concentrations would make active resistance and adequate decision-making difficult or impossible, which could provide a decisive advantage in conducting counter-terrorist operations.
In 1986, a symposium was held in Maryland dedicated to issues of chemical incapacitant against terrorists and aircraft hijackers. The chief anesthesiologist of the University of Utah, T. Stanley, mentioned here repeatedly, made an unexpected proposal — in his opinion, xenon was well suited for effectively neutralizing hijackers on aircraft, capable of quickly and without serious consequences putting everyone in the cabin to sleep. After the operation ended, it would be sufficient to provide them with access to fresh air for rapid awakening. However, with xenon priced at 10 dollars per liter, the amount of gas needed for the operation would cost several million dollars. The idea had to be abandoned[33].
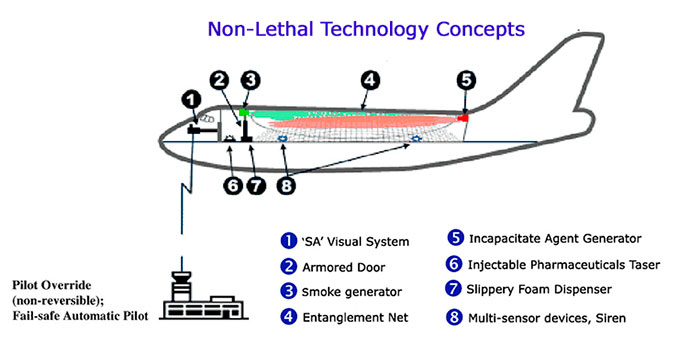
The possibility of using anesthetics to fight aircraft hijackers was discussed again in the early 2000s. In 2001, at a briefing for the International Air Line Pilots Association (ALPA), a concept was presented for an aircraft hijacking countermeasure system in which the passenger cabin and pilot cockpit had separate isolated air supply systems, and in case of terrorists in the cabin, they, along with passengers, could be put to sleep using aerosol or gaseous anesthetic[45]. After the September 11, 2001 terrorist attacks, this idea was further developed and planned to include remote flight control and landing from the ground, armored doors, movement-restricting nets, smoke and adhesive foam generators, sirens, and of course, sleeping agents not only in aerosol form but also in "flying syringes"[46].
In May 2002, at hearings in the US Senate dedicated to the use of non-lethal technologies for aviation security, National Institute of Justice Director Sarah V. Hart noted that
"anesthetics or calmative chemicals could, in principle, be developed into a system whereby they could be remotely released into the cabin in order to incapacitate all passengers, and the hijackers, until the plane can be landed safely. Chemical systems of this type have not been employed in the field, however, and remain under study or in development. Also, the effects of these chemicals are not rapid and so may not work fast enough to thwart an attack. Chemical agents used in the cabin may also create unacceptable risks to the health of vulnerable passengers (e.g., infants and those with asthma or other respiratory problems). Finally, the use of these weapons could prevent other passengers from assisting in immobilizing or restraining hijackers"[34].
Less than six months after this report, during the hostage rescue operation at Dubrovka in Moscow, narcotic gas was used, which killed 130 people. After this tragic incident, interest in developing narcotic incapacitants noticeably decreased, and some countries completely abandoned their development.
In Russia, xenon was widely used in sports medicine. Xenon inhalations increase the production of erythropoietin — a hormone that stimulates red blood cell production, leading to reduced hypoxia levels, increased endurance, and adaptation to physical and mental stress. During the 2004 and 2006 Olympics, 75% of Russian Olympic medalists inhaled oxygen-xenon mixture[58]. In 2014, the World Anti-Doping Agency (WADA) announced a ban on the use of xenon in sports.
There is no doubt that xenon will be used not only in sports medicine but also in military medicine. Methodological recommendations for xenon use were developed by the State Research and Testing Institute (of Military Medicine)[59], the production of portable inhalation devices involves the "Military-Industrial Company" and "Almaz-Antey Concern"[58], and military pilots participated in testing[60].
In Russia, other unusual applications for xenon have been found. Commercial clinics promise to use xenon to relieve stress, depression, and hangovers, increase sexual activity, and improve memory and thinking[57]. For example, in xenon therapy for menopause, "the patient experiences lightness, bliss, and a sense of enlightenment. It is precisely these sensations, close to a state of 'divine ecstasy,' that, as doctors have proven, have a healing effect on the entire body, restoring the function of all vital organs in women"[56].
But Russian researchers have gone even further. They propose abandoning complex and bulky inhalation equipment and adding xenon to food products such as cream or butter (although only 40 ml of xenon can dissolve in a glass of cream)[61] and even to ointments and cosmetic preparations to introduce xenon through the skin[62].